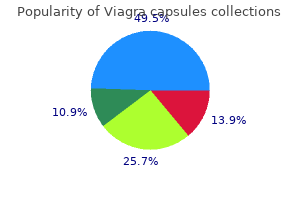
"Generic 100 mg viagra capsules free shipping, erectile dysfunction causes drugs".
By: D. Akascha, M.A.S., M.D.
Assistant Professor, A.T. Still University School of Osteopathic Medicine in Arizona
A three-dimensional reconstruction would show that the haversian canals are long branching channels running in the longitudinal axis of the bone and connecting extensively with each other and with the endosteal and periosteal surfaces by smaller channels (Volkmann canals) erectile dysfunction pills for heart patients order genuine viagra capsules on line. In this way the vessels in the haversian canals form a rich anastomotic network between the medullary and periosteal blood supply erectile dysfunction drug samples buy viagra capsules visa. However, it seems likely that at least the outermost layers of the cortex are normally also supplied by periosteal vessels, and if the medullary vessels are blocked or destroyed the periosteal circulation can take over entirely and the direction of blood flow is reversed. It is found where support matters most: the outer walls of all bones but especially the shafts of tubular bones, and the subchondral plates supporting articular cartilage. Between the lamellae lie osteocytes, bedded in lacunae which appear to be discrete but which are in fact connected by a network of fine canaliculi. The haversian canal offers a free surface lined by bone cells; its size varies, depending on whether the osteon is in a phase of resorption or formation. During resorption osteoclasts eat into the surrounding lamellae and the canal widens out; during formation osteoblasts lay down new lamellae on the inner surface and the canal closes down again. It shows the basic elements of compact bone: densely packed osteons, each made up of concentric layers of bone and osteocytes around a central haversian canal which contains the blood vessels; outer laminae of sub-periosteal bone; and similar laminae on the interior surface (endosteum) merging into a lattice of cancellous bone. At birth the cartilage model is complete and ossification has already begun at the centre of the diaphysis. After secondary ossification of the epiphyseal ends has begun, further growth in length takes place in the still cartilaginous zone between the extending area of diaphyseal bone and the epiphysis. In this way the still-cartilaginous zone between the ossifying diaphysis and the epiphysis gradually narrows down but does not disappear until late adolescence. This actively growing cartilage disc is called the physis, seated as it is between the epiphysis and the diaphysis. Coextensive with the epiphysis is a zone of resting chondrocytes in haphazard array. This merges into a proliferative zone in which the chondrocytes are lined up longitudinally; being capable of interstitial growth, they add progressively to the overall length of the bone. Close to the interface between cartilage and bone the cartilage becomes calcified (probably with the involvement of alkaline phosphatase produced by the hypertrophic cells); this zone of calcified cartilage finally undergoes osteoclastic resorption and, with the ingrowth of new blood vessels from the metaphysis, ossification. Woven bone is laid down on the calcified scaffolding and this in turn is replaced by lamellar bone which forms the newest part of the bone shaft, now called the metaphysis. It should be noted that a similar process takes place in the late stage of fracture repair. New bone is added to the outside by direct ossification at the deepest layer of the 121 7 7. Atlas of Orthopaedic Pathology: With Clinical and Radiological Correlations (2nd edition). During resorption each osteoclast forms a sealed attachment to the bone surface where the cell membrane folds into a characteristic ruffled border within which hydrochloric acid and proteolytic enzymes are secreted. At this low pH minerals in the matrix are dissolved and the organic components are destroyed by lysosomal enzymes. Calcium and phosphate ions are absorbed into the osteoclast vesicles from where they pass into the extracellular fluid and, ultimately, the blood stream. In cancellous bone this process results in thinning (and sometimes actual perforation) of existing trabeculae. During hyperactive bone resorption these processes are reflected in the appearance of hydroxyproline in the urine and a rise in serum calcium and phosphate levels. How else can a long bone retain its basic shape as the flared ends are constantly re-formed further and further from the midshaft during growth The internal architecture of the bone is also subject to remodelling, not only during growth but throughout life. Intramembranous periosteal new bone formation also occurs as a response to periosteal stripping due to trauma, infection or tumour growth, and its appearance is a useful radiographic pointer. Although it has Epiphyseal artery 7 Reserve cells Proliferative cells Metabolic and endocrine disorders Hypertrophic cells Degenerate cells Calcified zone Vascular invasion Ossification 7. Prompted by the osteoblasts, osteoclasts gather on a free bone surface and proceed to excavate a cavity.
For pockets 1 to 3 mm and 4 to 6 mm there was no difference in pocket reduction maintenance erectile dysfunction doctor montreal viagra capsules 100mg fast delivery. For attachment there was no difference in 1 to 3 mm probing depths and in 4 to 6 mm pockets impotence quotes cheap viagra capsules 100mg line, lower gingivitis scores had better gain the first 2 years but thereafter no difference was recorded. For 7 to 12 mm pockets, the lower gingivitis scores seemed to result in better probing levels and attachment gain for the first 3 years but this was not maintained throughout the experiment. The severity of gingivitis did not affect the maintenance of pocket depth reduction or clinical attachment levels. Patients with advanced periodontal disease were entered into a split mouth design to compare the results of subgingival debridement performed in conjunction with a modified Widman flap or scaling and root planing alone. Attachment levels improved following non-surgical therapy at 6 and 12 months, but at 24 months returned to baseline values. When comparing single-rooted to multi-rooted teeth, there was a trend for slightly better results for single-rooted teeth. These similar results can be maintained over time in patients with proper oral hygiene levels. Probing depths shallower than the critical probing depth tend to lose attachment following the procedure. The results also showed that the level of oral hygiene established during healing and maintenance is more critical for the resulting probing depths and attachment levels than the mode of treatment used. Sites with initial probing depth exceeding 3 mm responded equally well to non-surgical and surgical treatment. One side of both the maxilla and the mandible were treated with modified Widman flap. Patients were recalled every 2 weeks, and examination was performed at 3 and 6 months after the completion of treatment. Lateral incisors, canines, and premolars in the maxilla and mandible in 16 patients diagnosed with advanced periodontitis were used for study. The plaque index and bleeding on probing were assessed prior to and 3, 6, and 12 months after treatment. Probing depths and clinical attachment levels were assessed prior to and 1 year after treatment. Radiographs were taken using the bisecting angle technique before and 1 year after treatment, and the bone level was expressed as a percentage of the distance from the apex of the tooth to the normal bone level. Angular bony defects corresponding to 15% or more of the distance between the normal level of the bone and the apex of the involved tooth were located. Sixteen (16) patients with advanced periodontitis were subjected to supra- and subgingival scaling and oral hygiene instructions. Patients were then recalled regularly for the next 5 years Surgical and non-surgical treatment resulted in pocket reduction which was maintained over the 5 years. No correlation was found between oral hygiene and recurrence of periodontitis, suggesting subgingival scaling at frequent recalls is an important factor in halting the progression of disease. The results reported are essentially the same as those reported by the university studies, thus confirming the validity of university research and its applicability to the private practice setting. The study population consisted of 16 patients with 2 or more sites with > 6 mm of clinical attachment loss in the posterior dentition. All patients had a baseline examination including the plaque index, gingival index, probing depth, clinical attachment levels, mobility, and furcation status. The clinical attachment level measurements were classified as 0 to 2 mm; 3 to 5 mm; and > 6 mm. Quadrants were randomly assigned to 1 of 3 treatment groups: scaling and root planing, modified Widman flap surgery, or osseous surgery. At 1 year post-treatment, osseous and modified Widman surgery had significantly greater probing reduction when compared to scaling and root planing. For pockets > 7 mm, osseous and modified Widman surgery had significantly greater reduction when compared to scaling and root planing. For pockets 1 to 3 mm, osseous surgery had significantly greater clinical attachment loss when compared with scaling and root planing. The results indicate that at 1 year, scaling and root planing, osseous surgery, and the modified Widman procedure were equally effective in treating moderate to advanced periodontitis. Sixteen (16) patients with moderate periodontitis were treated in private practice by periodontists highly competent in performing scaling and root planing, modified Widman flap, and osseous surgery. At the 5-year evaluation, plaque and gingival indices were reduced and maintained throughout the study with no difference between treatment methods; 1 to 3 mm probing depths increased insignificantly but were stable at 3 years; 4 to 6 mm pockets were reduced significantly, but diminished over time.
Buy 100 mg viagra capsules fast delivery. Silas Marner Audiobook by George Eliot | Audiobook with subtitles.

He states that his worry is interfering with his ability to complete work assignments erectile dysfunction pills free trial 100mg viagra capsules with amex. He states that he counts to 100 repetitively in order to distract himself from this worry erectile dysfunction keeping it up viagra capsules 100 mg amex. Anterior capsulotomy and/or cingulotomy are indicated and demonstrated effective for pts with what severe incapacitating disorder Pt is hoarding, home filled with filth, acknowledges is she is keep a lot of things (hoarding) Which condition is least likely to respond to hypnosis Pt denies fear of germs or any obsessive thoughts, cannot explain continuous washing. The surgeon believes that none of his complaints have been satisfactorily resolved. He has become more unforgiving and isolated: (2x) Borderline patient pulling away from a relationship due to growing up in abusive household is stuck in which stage 30 yo is pushed by family to get help for isolation she is uncomfortable around others and have problems making friends unless convinced they will accept her. She thinks others are highly critical of her and only has 2 close friends from childhood and has never dated. Her history is significant for promiscuity, spending sprees, tumultuous relationships, unstable self-image, and occasional use of cocaine. During and emotional break-up with her last boyfriend, which remitted after a 2-day admission to the psych unit. Classmates have described bizarre behavior, such as counting loudly or repeating words silently. He does not want to follow others rules but his owns, he believes nobody understands him and are against him. Which personality disorder is characterized by a style of speech that is excessively impressionistic and lacking in detail Pt becomes panicky and distressed every time psychiatrist goes on vacation, this pattern is most likely a characteristic of: Pt with histrionic personality d/o storms in his psychodynamic session and a few minutes late, clearly in rage. Which personality d/o should be in the dif dx of agoraphobia: 23 y/o M w/ Borderline. Pt repeatedly becomes distressed after what seems, even to the pt, to be minor disappointments. A therapist utilizing self-psychology would be most likely to interpret this as due to A family history of which of the following personality d/o is most strongly associated with this dx There is increased risk of schizophrenia with this personality disorder Which intervention is helpful in dealing with a borderline pt on a medical ward Pts that "cut" as a form of self-mutilation typically: Which test to confirm personality disorder Obsessive-compulsive Personality Disorder Has gotten feedback that she spends too much time organizing and highlighting her notes. A fear of choking while eating and a wish to avoid foods that might cause choking developed. Upon questioning, pt admits to washing the hands many times a day because "I work in a hospital cafeteria and am intensely afraid of contracting a flesh-eating bacterial infection. Dx: Avoids interpersonal situations due to anxiety and panic attacks 28 y/o M episodic anxiety, palpitations, flushing, shaking, chest tightness. Embarrassed, afraid to go to work, avoiding people: Most effective approach in behavioral treatment of phobias: this medication is commonly used in social phobia associated with performance situations, shortly before exposure to a phobic stimulus In addition to these symptoms, what is required for diagnosis of Schizoaffective disorder Talks to self, talks about being controlled by aliens, believes aliens are putting thoughts in his head. Poverty of speech and poverty of content are aspects of which of the following conditions Pt also has unusual movements of arms at times, flap and wave on their own accord. Though recent research has demonstrated that the blunted emotional expression in schizophrenia does not imply that a patient is anhedonic, individuals with schizophrenia do experience loss of interest or pleasure associated with After several days pt has muscle tremor, ataxia, twitching, diarrhea, restlessness, vomiting, polyuria, and stupor.
After nerve regeneration or repair erectile dysfunction causes generic 100mg viagra capsules with mastercard, a proportion of proximal sensory axons will fail to reach their appropriate sensory end-organ; they will either have regenerated down the wrong Schwann-cell tube or will be entangled in a neuroma at the site of injury erectile dysfunction yahoo answers order viagra capsules. Therefore, two-point discrimination (measured with a bent paper clip and compared with the opposite normal side) gives an indication of how completely the nerve has recovered. Static two-point discrimination measures slowly adapting sensors (Merkel cells) and moving two-point discrimination measures rapidly adapting sensors (Meissner corpuscles and pacinian corpuscles). They are more useful in nerve-compression syndromes, where individual receptors fail to send impulses centrally; two-point discrimination is preserved because the innervation density is not affected. Fine nylon monofilaments of varying widths are placed perpendicularly on the skin and the size of the lightest perceptible filament is recorded. Locognosia is the ability to localize touch and can be tested with a standardized hand map. The patient is blindfolded and instructed to pick up and identify nine objects as rapidly as possible. Exploration is indicated: (1) if the nerve was seen to be divided and needs to be repaired; (2) if the type of injury. Vascular injuries, unstable fractures, contaminated soft tissues and tendon divisions should be dealt with before the nerve lesion. The incision will be long, as the nerve must be widely exposed above and below the lesion before the lesion itself is repaired. If microsurgical equipment and expertise are not available, then the nerve lesion should be identified and the wound closed pending transferral to an appropriate facility. A clean cut nerve is sutured without further preparation; a ragged cut may need paring of the stumps with a sharp blade, but this must be kept to a minimum. The stumps are anatomically orientated and fine (10/0) sutures are inserted in the epineurium. Sufficient relaxation of the tissues to permit tension-free repair can usually be obtained by positioning the nearby joints or by mobilizing and re-routing the nerve. These injuries are best dealt with in specialized centres, where primary grafting or nerve transfer can be carried out. If a tourniquet is used it should be a pneumatic one; it must be released and bleeding stopped before the wound is closed. The limb is splinted in a position to ensure minimal tension on the nerve; if flexion needs to be excessive, a graft is required. The options must be carefully weighed: if the patient has adapted to the functional loss, if it is a high lesion and re-innervation Primary repair A divided nerve is best repaired as soon as this can be done safely. Primary suture at the time of wound toilet has considerable advantages: the nerve ends 274 is unlikely within the critical 2-year period, or if there is a pure motor loss which can be treated by tendon transfers, it may be best to leave well alone. Excessive scarring and intractable joint stiffness may, likewise, make nerve repair questionable; yet in the hand it is still worthwhile simply to regain protective sensation. The lesion is exposed, working from normal tissue above and below towards the scarred area. When the nerve is in continuity it is difficult to know whether resection is necessary or not. The stumps may be brought together by gently mobilizing the proximal and distal segments, by flexing nearby joints to relax the soft tissues, or (in the case of the ulnar nerve) by transposing the nerve trunk to the flexor aspect of the elbow. It is also possible to use free vascularized grafts for certain brachial plexus lesions. Nerve transfer In root avulsions of the upper brachial plexus, too proximal for direct repair, nerve transfer can be used. The spinal accessory nerve can be transferred to the suprascapular nerve, and intercostal nerves can be transferred to the musculocutaneous nerve. If biceps has failed because too much time has passed since the injury, an entire muscle (gracilis or latissimus dorsi) can be transferred as a free flap, attached between elbow and shoulder and then innervated by joining Nerve guides It is now apparent that nerve gaps can regenerate through a tube which excludes the surrounding tissue from each end. The tubes can be autogenous vein, freeze-dried muscle, silicone or metal; soluble guides (flexible at body temperature) which dissolve over weeks or months are also used. This technology offers a simple way of avoiding a nerve graft yet achieving results which are at least as good in both digital nerves and probably in main trunks. The donor muscle should be: expendable powerful enough an agonist or synergist the recipient site should: be stable have mobile joints and supple tissues the transferred tendon should be: routed subcutaneously placed in a straight line of pull capable of firm fixation the patient should be: motivated able to comprehend and attend hand therapy Nerve grafting Free autogenous nerve grafts can be used to bridge gaps too large for direct suture.