"Purchase trazodone without prescription, medications adhd".
By: R. Hector, M.S., Ph.D.
Medical Instructor, Case Western Reserve University School of Medicine
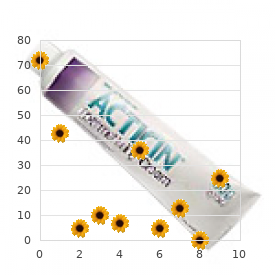
Visualization of these configurational changes (reduced size medications for ibs purchase trazodone pills in toronto, nodularity treatment action campaign buy trazodone on line amex, calcification) by computed tomography can be extremely useful in the diagnosis of analgesic nephropathy. A decrease in kidney size combined with bumpy contours of both kidneys provides a diagnostic sensitivity of 90% and a specificity of 95%. The additional finding of evidence of papillary necrosis increases the specificity to 97%, with a positive predictive value of 92%. The lesions of analgesic nephropathy are patchy and slowly progressive, remain asymptomatic, and will usually go undetected until the onset of azotemia. They should be considered in anyone with sterile pyuria, reduced concentrating ability, and a distal tubular acidifying defect, effects that are evident at levels of mild renal insufficiency and gradually become more pronounced and clinically evident as renal function deteriorates. Proximal tubular function is preserved in those with mild renal insufficiency, but it becomes abnormal with advanced renal failure. The presence of any tubular dysfunction, even with normal blood urea nitrogen and serum creatinine levels, should always lead to careful questioning about analgesic use and possible urinary screening for analgesic metabolites. Analgesic nephropathy is more common in women, in those who are 30 to 50 years old, and in regions where over-the-counter sale of analgesic mixtures is high. Certain personality features (dependency, moodiness) and clinical complaints (headache, musculoskeletal pain, arthralgias) characterize individuals prone to analgesic use. Anemia and peptic ulcer symptoms caused by the gastrointestinal effects of analgesics are common findings and may be the initial complaint in some. Those who do not discontinue analgesic Figure 107-2 Configurational changes (reduced volume, nodularity, calcification) observed on computed tomographic scanning of the kidney in analgesic nephropathy. Monitoring for uroepithelial malignancies is important, even after analgesic discontinuation, because as many as 10% of chronic analgesic users are prone to this otherwise rare form of cancer. Although discontinuation of chronic analgesic use is important, avoidance of their use in combination is by far more essential. In countries in which over-the-counter sale of analgesic mixtures has been banned, a reduced incidence of analgesic nephropathy has been noted. Aspirin alone in therapeutic doses does not impair renal function in patients with normal renal function. However, aspirin overdosage may impair renal function, especially in those with renal disease. Clinical evidence suggesting that the habitual use of acetaminophen alone causes the clinical entity of classic analgesic nephropathy is negligible. Acetaminophen has been preferentially recommended to patients with renal failure because of the bleeding complications associated with aspirin in these individuals. As such, its association with renal failure may well be an epiphenomenon rather than one of causal association. There is no evidence that the occasional use of acetaminophen causes renal injury or is detrimental to those with renal disease. The most common side effect of lithium is vasopressin-resistant nephrogenic diabetes insipidus, which is often accompanied by additional evidence of distal tubular dysfunction, such as a mild form of distal renal tubular acidosis and sodium wasting. Cyclosporine-mediated vasoconstriction of the microvasculature accounts for a characteristic occlusive arteriolopathy and subsequent tubular epithelial cell injury. A principal side effect of antineoplastic agents is direct tubular toxicity with the clinical features of acute renal failure. An invariable concern in all such cases is the consequently prolonged half-life of the agents administered and their increased tendency to systemic toxicity. Major sources of lead exposure are lead-based paints, lead leached into food during storage or processing, particularly in home-brewed illegal alcoholic beverages (moonshine), and increasingly, environmental exposure (gasoline, industrial fumes). This insidious accumulation of lead has been implicated in the etiology of a syndrome of hyperuricemia, hypertension, and progressive renal failure. As might be expected from its association with elevated blood pressure, hypertensive vascular changes are a prominent feature of the kidney in these cases. Acute lead intoxication is rare but may be encountered after accidental ingestion, usually by children. Its principal manifestations are abdominal colic, hemolytic anemia, and encephalopathy. Exposure to cadmium results in the preferential accumulation of cadmium in the proximal tubule, where it is retained with a rather long biologic half-life of at least 10 years. Tubular degeneration, interstitial fibrosis, and mononuclear cell infiltration are central components of injury to the kidney by vascular diseases that affect the intrarenal circulation.
Anomalies of the Sinuses of Valsalva and Coronary Arteries Sinus of Valsalva Aneurysms At the base of the aortic root medicine head discount trazodone 100mg mastercard, the aortic valve cusps are attached to the aortic wall medications elderly should not take buy trazodone 100 mg online, above which three small pouches, or sinuses, are seated. The right coronary artery originates from one sinus and the left main coronary artery from a second; the third is called the non-coronary sinus. A weakness in the wall of the sinus can result in aneurysm formation with or without rupture. Rupture typically occurs into the right heart at the right atrial or ventricular level with a resulting large left-to-right shunt driven by the high aortic pressure. A previously asymptomatic young man typically has chest pain and rapidly progressing shortness of breath sometimes after physical strain. Even if the communication is between the aorta and the right heart, biventricular failure is not unusual. A murmur of aortic insufficiency secondary to damage to the adjacent aortic valve may be superimposed. The chest radiograph shows volume overload of both ventricles with evidence of shunt vascularity and pulmonary venous congestion. Cardiac catheterization can verify the integrity of the coronary artery adjacent to the ruptured aneurysm. Even though symptoms may abate as the heart dilates, progressive cardiac decompensation typically results in death within 1 year of the rupture. Coronary Artery Fistulas Fistulas arise from the right or left coronary arteries and in 90% of cases drain into the right ventricle, the right atrium, or the pulmonary artery in order of decreasing frequency. Typically, young patients are asymptomatic, but supraventricular arrhythmias are seen with progressive dilatation of the intracardiac chambers. Angina can occur as the fistula creates a coronary steal by diverting blood away from the myocardium. A continuous murmur heard in a young, otherwise normal acyanotic, asymptomatic patient should raise suspicion of the diagnosis. Most fistulas are associated with a small shunt and hence the murmur is often less than grade 3 and is heard in the precordial area. Unless the shunt is large, the electrocardiogram is normal, as is the chest radiograph. Percutaneous transcatheter closure with coil embolization is preferred, but surgical ligation is also an alternative. Anomalous Origin of the Coronary Arteries the left main coronary artery normally arises from the left sinus of Valsalva and courses leftward, posterior to the right ventricular outflow tract. The right coronary artery arises from the right sinus of Valsalva and courses rightward to the right ventricle. The most common anomaly is ectopic origin of the left circumflex artery from the right sinus of Valsalva, followed by anomalous origin of the right coronary artery from the left sinus and anomalous origin of the left main coronary artery from the right sinus. If the anomalous coronary artery does not course between the pulmonary artery and aorta, the prognosis is favorable. Risks of ischemia, myocardial infarction, and death are greatest when the left main coronary artery courses between both great vessels. If both the right and left arteries originate from the pulmonary trunk, death usually occurs in the neonatal period. If only the left anterior descending coronary artery originates from the pulmonary trunk, the rate of survival to adulthood is approximately 10%, depending on the development of collateral retrograde flow to the anomalous artery from a normal coronary artery. This collateral flow may cause a continuous murmur along the left sternal border, congestive heart failure from the large shunt, and a coronary steal syndrome as blood is diverted away from the normal artery. A single coronary ostium can provide a single coronary artery that branches into right and left coronary arteries, the left then giving rise to the circumflex and the anterior descending arteries. The coronary circulation is functionally normal unless one of the branches passes between the aorta and the pulmonary artery. For an anomalous coronary artery that originates from the pulmonary artery, surgical reimplantation into the aorta is preferred. For an anomalous artery that courses between the pulmonary artery and aorta, a bypass graft to the distal vessel is preferred.
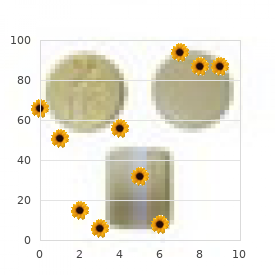
The two "popular" radiologic signs of left atrial enlargement-a double contour within the right cardiac border and elevation of the left main bronchus-are both accurate when present treatment bulging disc discount trazodone online visa, but are insensitive schedule 8 medicines generic 100 mg trazodone otc. To produce a discernible margin within the cardiac silhouette in the frontal projection, the thickness of the heart must increase sharply at some point. This increase in thickness occurs in mitral disease when the left atrium enlarges and protrudes posteriorly Figure 41-3 Left atrial enlargement in mitral valve disease. A, Patient 1: the enlarged left atrium causes the central portion of the cardiac silhouette to be abnormally dense. The right border of the atrium is seen within the right side of the cardiac silhouette. The region of the left atrial appendage (white arrow) is slightly concave because this structure was resected at a previous mitral commissurotomy. B, Patient 2: the enlarged left atrial appendage bulges from the left side of the heart (white arrow), whereas the body of the atrium (arrowheads) extends beyond the right atrium to form a part of the right heart border. No double density is seen within the heart, and the left main bronchus (small arrows) is not elevated. The right border of the left atrium is then silhouetted where it abuts the right lung and its contour is seen within the cardiac silhouette. Conversely, when the right atrium also enlarges, as is common in long-standing Figure 41-5 Left ventricular aneurysm. A bulge on the lower portion of the left cardiac border, formed by the anterolateral wall of the left ventricle, represents a ventricular aneurysm. Thus, the double contour is not seen with mild left atrial enlargement or in severe cases of mitral disease. Furthermore, the radiologic technique used for chest films is chosen to provide optimal images of the lungs. The heart, when enlarged, is underexposed, and the double contour may not be seen within its opaque silhouette. For the same reason, the position of the left main bronchus often cannot be clearly visualized through the mediastinal shadow. A more sensitive sign of left atrial enlargement in the frontal projection is dilation of the left atrial appendage. The appendage extends anteriorly from the atrium along the left side of the heart, below the level of the pulmonary artery. It forms the part of the left heart border between the pulmonary artery segment and the left ventricular segment. The shape of the dilated left ventricle depends to a large extent on the underlying cause. When it is due to insufficiency of the aortic or mitral valve, the ventricle elongates and its apex is displaced downward, to the left, and posteriorly. When the dilatation is due to coronary artery disease or primary myocardial disease, the ventricle tends to assume a more globular shape. In the lateral view, the downward extension of the enlarged left ventricle covers more of the vena caval shadow than normal, and the crossing point of their posterior borders occurs nearer to the diaphragm than normal. Unfortunately, the usefulness of this sign is limited because even slight rotation of the patient from the true lateral position distorts the apparent relationship between the two structures. Enlargement of the left ventricle produces a smoothly curved dilatation of the lower portion of the cardiac silhouette. A localized bulge in this contour most often represents a ventricular aneurysm. Dilatation of the left ventricle is usually associated with elevation of left ventricular end-diastolic pressure. The latter increases the resistance to left atrial emptying and can result in dilation of the atrium. Therefore, left atrial enlargement in the Figure 41-6 Right ventricular enlargement seen in a patient with resistive pulmonary hypertension secondary to an atrial septal defect. The main pulmonary artery (arrow) and the right pulmonary artery are markedly dilated. The left pulmonary artery was also dilated but is hidden by the heart in this view. The sudden "cutoff" of the vascular shadows just beyond the hila is characteristic of resistive pulmonary hypertension.
The presence of calcification in at least 10 to 20% of the nodule near its center is the most reliable indicator of a benign lesion medications given for bipolar disorder order generic trazodone from india. However calcification of a solitary nodule is not specific for benign disease medications and side effects order trazodone online, as a cancer can develop within a scar or granuloma. A thorough review and analysis of the relationship of pulmonary symptoms to clinical and physiologic abnormalities in a range of pulmonary disorders. An informative review of the diagnostic role of positron emission tomography in relation to other tumor imaging modalities. Approach to the clinical and radiographic evaluation of patients with common pulmonary syndromes. A thorough discussion of the use of history, physical examination, and radiologic findings for differential diagnosis of lung diseases. In addition, the respiratory system carries out a large number of other ventilatory-related and nonventilatory functions. The complex effects of lung structure on its gas exchange and nonventilatory functions are critical to understanding how the lung responds to both intrapulmonary and systemic diseases. The nasopharynx plays a critical role in humidifying inhaled gases and in clearing particles and reactive substances contained in those gases. In addition to contributing to the senses of smell and taste, the nasopharynx removes a large fraction of inhaled particles and reactive gases. Turbulent gas flow past the nasal turbinates and the right-angle turn at the posterior pharynx cause impaction of most large particles before inhaled gas enters the trachea. In addition, very highly soluble or reactive gases may be almost completely removed by the nasopharynx. Lymphoid tissue at the posterior pharynx plays a role in immune processing at this critical junction of the body with its external environment. The posterior portion of the trachea, representing the membranous portion or open part of the cartilaginous rings, contains the trachealis muscle. The trachea divides into two main-stem bronchi, which then rapidly divide in an irregular dichotomous pattern into progressively smaller bronchi. Cartilaginous support surrounding or partly surrounding bronchi continues for a number of generations, at which point the airways are termed bronchioles. As the size of the cartilage decreases in smaller bronchi, the relative mass of smooth muscle becomes more prominent, and these medium-sized bronchi can be a significant site of bronchoconstriction. Smooth muscle becomes more scarce, as it extends into the bronchioles and is virtually absent from terminal bronchioles. The shortest path from the trachea to a terminal bronchiole involves approximately seven divisions and has a total length of 7 to 8 cm. The longest pathway would encounter approximately 25 branch divisions and have a total length of more than 22 cm. The cross-sectional area of each daughter branch is decreased, but the increasing number of branches leads to an increase in the total cross-sectional area as air moves deeper into the lung. The increase in airway cross-sectional area is nearly exponential and leads to a fall in airway resistance distal to the conducting airways. As a result, the primary site of air flow resistance is in the large, central airways. Gas flow rates also slow as the cross-sectional area increases and the flow pattern becomes less turbulent and more laminar. The final airway segments are termed terminal bronchioles, which then branch into two to four respiratory bronchioles (airway segments with alveolar or gas exchange outpockets) before entering alveolar ducts. The terminal bronchioles are approximately 250 mum in internal diameter, do not have smooth muscle, and are covered only with a thin, serous fluid coat. They are not normally a site of significant airway resistance but may become so during a number of disease processes. The airways and large vessels in the lung make up about 10% of the substance of the lung and account for about 25% of the lung cells. More than 40 different cell types are found in the lungs, 383 representing virtually every major class of tissue. The most common type of cell in the lung is the capillary endothelial cell, which represents almost 40% of the cells in the alveolar gas-exchange region.
Discount trazodone line. What is Pneumonia? | Pneumonia: types causes and treatment | Dr. P.V. Keshav Gurnada Kumar.